As Joe Rogan told it, President Donald Trump jumped at the chance to facilitate regulatory approval of ibogaine and other psychedelics that have shown promise as psychotherapeutic catalysts. After the hugely popular, politically eclectic podcaster texted the president information about ibogaine, Rogan recalled, Trump replied: “Sounds great. Do you want FDA approval? Let’s do it.”
Rogan, who endorsed Trump in the 2024 election, told that story on April 18 as Trump signed an executive order instructing the Food and Drug Administration (FDA) to accelerate the review process for “appropriate psychedelic drugs,” including ibogaine, and provide “at least $50 million from existing funds” to state programs investigating their potential. The FDA also is supposed to collaborate with the Department of Veterans Affairs on clinical trials.
In addition to Rogan’s role as a popularizer of psychedelic research, the signing ceremony highlighted the experiences of veterans who credit ibogaine-assisted insights with turning around lives derailed by psychological trauma, brain injuries, and addiction. The veteran angle goes a long way toward explaining why this cause has been embraced by the Trump administration and by conservative Republicans such as former Texas Gov. Rick Perry, Texas Rep. Dan Crenshaw, the Texas legislators who approved funding for ibogaine studies in 2025, and the Utah legislators who overwhelmingly backed psychedelic research in 2022.
Trump’s order noted an upswing in the U.S. suicide rate during the last two decades, emphasizing that “veterans often suffer in greater measure from this tragedy.” Former Navy SEAL Marcus Luttrell, whose Afghanistan memoir inspired the 2013 movie Lone Survivor, thanked Trump for his executive order, saying, “You’re going to save a lot of lives with it.”
Luttrell, who underwent ibogaine therapy at a clinic in Mexico, said “it absolutely changed my life for the better.” His twin brother, Rep. Morgan Luttrell (R–Texas), also a former Navy SEAL, likewise calls his experience with ibogaine “one of the greatest things that ever happened to me.”
In accordance with Trump’s order, then–FDA Commissioner Marty Makary said his agency had approved the first human trial of ibogaine in the U.S., testing it as “a potential treatment for alcohol use disorder.” Other psychedelics, including psilocybin and MDMA, are further along. And six days after Trump signed his order, the FDA issued “national priority vouchers” for psilocybin as a treatment for depression and methylone, which is similar to MDMA, as a treatment for post-traumatic stress disorder.
The FDA had already designated psilocybin and methylone as “breakthrough” therapies, which is supposed to speed up the review process. The vouchers go further, promising an “ultra-fast timeline” of one to two months, rather than six months or more, after the requisite studies are completed.
The post Trump's Embrace of Psychedelic Therapy Could 'Save a Lot of Lives' appeared first on Reason.com.
]]>
I was 22 when my grandmother forgot me.
It took her 12 years to die from Alzheimer’s. It started with little things, like where her glasses were or what day it was. Soon she didn’t know who I was. For a while, she addressed me as her son, but then, as the disease ate away more of her mind, she forgot him too. Then I was the young, handsome version of her husband, until he too faded away. After a while, I was just a nice young man who came to visit her.
The rest of the time, she was afraid: waking up in an unfamiliar world, surrounded by people she’d never met, confused that she wasn’t back home in Minnesota, where she’d grown up. It hit my mom the hardest. She did everything she could to take care of her own mother, watching the brilliant, kind woman she knew rot into a husk of her former self.
My grandmother died on Christmas Eve. As sad as it was, it was a blessing for my mom, who was finally freed from her duty of watching the woman she loved the most waste away.
The Alzheimer’s Researcher Who Became a Poster Child for Academic Fraud
Sylvain Lesné, a neuroscientist at the University of Minnesota, published a paper in Nature in 2006 claiming to identify a specific amyloid beta protein assembly as the direct cause of memory impairment in Alzheimer’s. This reinvigorated the amyloid hypothesis at a moment when skepticism about it was ramping up. The National Institutes of Health (NIH) devoted $1.6 billion to projects that mention amyloids in 2022 alone, nearly half of all federal Alzheimer’s funding that year. Lesné was a star.
But there were rumblings. Numerous amyloid drugs made it to trials with billions invested by pharmaceutical companies. They failed repeatedly. A question arose in the pharmaceutical community: How can this be right? How can the trials keep failing if the underlying research is correct?
In 2022, the Vanderbilt neuroscientist Matthew Schrag uncovered evidence that images in Lesné’s paper had been manipulated. Science magazine found more than 20 suspect papers by Lesné, with over 70 instances of possible image tampering. Nature retracted the paper in June 2024. Every author except Lesné signed the retraction. Lesné himself resigned from his tenured position at the University of Minnesota on March 1, 2025, three years after his fraud was exposed.
More news and details trickled out over time. Charles Piller’s 2025 book Doctored talks about the Amyloid Mafia, a nickname for a network that had prioritized novelty over replication and marginalized dissenters for decades. Anyone questioning the amyloid gospel was pushed out and watched their funding vanish.
When I first picked up that Science article, I hadn’t considered academic fraud as something that was real and widespread. As I thought about it more, I was filled with a deep, bitter hatred. For his own pride, greed, and acclaim, this man had doomed millions of people like my grandmother to slow, horrible deaths and millions more like my mom to agonizing years as caregivers.
Lesné resigned, but was still rich. None of his grant money was clawed back. The system that was supposed to catch this—peer review, university compliance, journal editorial boards—failed repeatedly for years.
How Much Academic Literature Is Made Up?
Lesné was not a lone bad apple. The rot and corruption of academic research are systemic and structural. Daniele Fanelli’s 2009 meta-analysis of survey data in PLOS One showed that approximately 2 percent of scientists self-reported fabrication or falsification—and 14 percent reported witnessing it in colleagues. Self-reports mark the floor, not the ceiling.
J.B. Carlisle’s 2021 paper, “False individual patient data and zombie randomised controlled trials submitted to Anaesthesia,” showed that out of 153 trials with individual patient data available, 44 percent had untrustworthy data and 26 percent were zombie trials animated entirely by false data. In a 2025 PNAS study, researchers estimated that the number of fraudulent publications is doubling every 1.5 years, while legitimate publications double every 15.
At least 400,000 papers published from 2000 through 2022 showed signs of coming from paper mills. Former BMJ editor Richard Smith asked, “Is it time to assume health research is fraudulent until proven otherwise?” A 2015 Lancet comment by Richard Horton put it bluntly: “Much of the scientific literature, perhaps half, may simply be untrue.”
The Peer Review System Is Susceptible to Scientific Fraud
Mancur Olson’s The Logic of Collective Action explains why systems that everyone knows are broken continue. When the benefits of cheating are concentrated in a small group but the costs are distributed across a vast population, the cheaters organize and the victims don’t.
Lesné captured millions of dollars in grants, plus tenure, prestige, and conference invitations. But the millions of Alzheimer’s patients and families, the wasted taxpayer money, and the honest researchers who could have gotten those grants instead—they all suffered for those benefits. None was hurt directly enough to trace culpability, but they suffered nonetheless.
Academia suffers from second-order Olson problems. Peer reviewers are unpaid volunteers with no upside for catching fraud and with significant social downsides for making accusations. University administrators have concentrated incentives to protect grant-winning faculty. The University of Minnesota investigation took roughly two and a half years and produced only a single resignation: Lesné’s. There were no legal consequences, no clawbacks.
The peer review process helps enable this fraud. The economist Bruce Yandle called it the “Bootleggers and Baptists” phenomenon: A group with strongly held moral beliefs will end up working with people interested in exploiting it financially. Self-righteous gatekeepers say peer review is required for integrity. As a byproduct, the publishing oligopoly extracts billions in profit by charging for access to taxpayer-funded research. Paper mills have become a shadow market worth, by one conservative estimate cited by Nature, hundreds of millions of dollars per year by publishing any slop they get their hands on, knowing that researchers desperate to publish would rather cheat than starve and that sociopaths would happily buy authorship with a credit card.
An entire extractive industry that charges universities to access their own faculty’s work, failing at its literal one job: integrity in publishing.
The system actively selects for corruption. The goals of individual scientists—getting published and getting grants—are structurally misaligned with the goals of science itself: the pursuit of truth. The Food and Drug Administration Amendments Act of 2007 legally required public posting of clinical trial results on ClinicalTrials.gov. A 2015 New England Journal of Medicine analysis showed only 13.4 percent compliance in reporting summary results within the required 12-month window. The government has the authority to fine violators up to $10,000 per day; it could have collected $25 billion according to a 2015 STAT investigation. But it collected essentially nothing, because the agency doesn’t want to fight the powerful institutions it regulates.
When institutional gatekeepers have failed, the answer is not yet more gatekeeping by corrupt watchers and underhanded dealers. It’s radical transparency and the free exchange of information.
Science must be a free market of ideas, but now it’s a cartel. NIH grant funding is centrally planned science. A small committee directs billions, yet is structurally incapable of knowing which directions are most promising.
Luckily for us, information wants to be free.
AI Can Empower Independent Scientists To Fight Academic Corruption
Professionalization and credentialism dominated science in the 20th century, suppressing independent research. But Charles Darwin was an amateur naturalist, Benjamin Franklin a printer, Michael Faraday a bookbinder. I believe the world is not only ready but eager for a new wave of citizen scientists, independent researchers, and curious minds to hunt through those monumental piles of data, to burn through corrupt and deceitful journals, and to replicate the most audacious claims in pursuit of truth.
It isn’t intelligence or motivation that limit independent research. The biggest limit is the labor cost of accessing, reading, cross-referencing, and synthesizing enormous bodies of literature. The advent of incredibly powerful AI has collapsed that cost by orders of magnitude. A motivated researcher with a ChatGPT Pro subscription can do in an hour what previously required months, a research team, and institutional library access.
The remaining limits are rigor, access to data, and the ability to conduct experiments. That’s where open infrastructure comes in, and that’s what I’m helping build today.
An acquaintance on X once told me that no one is translating Chinese research preprints to English. I smirked in disbelief. “There is literally no way that’s true,” I thought—and yet I looked, and it was. Thousands of Chinese preprints sat entirely untranslated with no real reference. A ripe opportunity to do something important was in front of me, and I decided to go and pick the low-hanging fruit.
ChinaRxiv.org now has 26,000 high-quality translated preprints, with the goal of continuing to expose information, to make it so researchers with high integrity have access to absolutely everything they can get their hands on to do their best work. If artificial superintelligence arrives soon, it probably won’t particularly care about what language any information is in—and as we train bigger and stronger models, getting information in datasets that are easily scrapable and accessible is a big win.
From there, a new opportunity emerged: Soviet-era Russian academic literature, a vast corpus of pre-1980s papers that were never translated into English. Through conversations on social media, I met some like-minded researchers and connected with the Research Revival Fund, sponsored by the Analogue Group. Together, we are getting ready to translate large stretches of previously untranslated Soviet academic papers.
There are entire research traditions in material science, theoretical physics, mathematics, and biology that were conducted in Russian but never entered the English scientific conversation. It’s still sitting there, untranslated, waiting to be found and introduced to the world.
The Real Victims of Corrupt Science, Slow Research, and Constrained Information
The victims of corrupt science and siloed information never know they were harmed. The child who dies because her cure was delayed by a few years never knows the hurt that she received. The researchers who didn’t get the grant for their novel idea because the cartel was funding their buddies on the backs of fraudulent graphs never knew they got screwed. In light of all this disappointment, we have a choice: Continue trusting failed institutions that are mired in corrupt incentive structures, or build a parallel world that routes around these gatekeepers. Let free information and free markets do what centrally planned science cannot, and let the best works survive.
Real people suffer and die when science is slow, when science is corrupt, when science is constrained. When you remove barriers to information and let individuals act on dispersed knowledge, you get outcomes no central planner could ever dream of.
The post How a Scientific Cartel Protects Fraudsters and Rakes in Billions of Taxpayer Dollars appeared first on Reason.com.
]]>
Over the last week, Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. has been defending his proposed budget for FY 2027 on Capitol Hill. Most lawmakers aren’t happy.
The budget seeks to cut HHS’ spending by 12.5 percent, or $15.8 billion, from FY 2026 levels. The largest named programmatic reduction is for the National Institutes of Health (NIH), which would see a $5 billion cut in spending (though its budget would still be roughly $41 billion), reducing the number of institutes and centers from 27 to 22. The proposed budget also calls for the elimination of the Low Income Home Energy Assistance Program, saving $4 billion, and consolidating several health offices into a new Administration for a Healthy America (AHA), which the HHS says will save $5 billion.
Kennedy defended this reorganization by telling the Senate Health, Labor, and Pensions Committee on Wednesday that when he came into office, HHS “had nine separate offices for women’s health, eight separate offices for minority health, 27 separate HIV programs, 59 behavioral health programs, 40 separate opioid programs, 42 maternal health programs, 41 chief information officers, 100 communications offices, 40 procurement departments, and dozens of IT departments. None of them talking to each other. And so it was a target-rich environment for reorganization to streamline the agency and make it more efficient.”
Ignoring the potential efficiency gains that these changes might bring, several lawmakers over the past week have decried the proposed budget. Sen. Patty Murray (D–Wash.) said cutting funding to NIH research will mean “delayed cures…cancelled studies…[and] no hope for patients who are fighting for their lives.”
Last week, Rep. Richard Neal (D–Mass.) told Kennedy that “the cuts that are being proposed to these initiatives are not helpful to the American family.” Similarly, Rep. Rosa DeLauro (D–Conn.), the ranking member of the House Appropriations Committee, said “We are not going to do that,” after listing some of the HHS’s proposed spending cuts.
This trepidation is unsurprising. Lawmakers have long argued that less federal spending on public health automatically leads to worse health outcomes, and that Washington’s current footprint is necessary and effective.
“Every time someone advocates a government activity…they say this is going to save lives. Almost never do they provide evidence establishing that,” Michael Cannon, director of Health Policy Studies at the Cato Institute, tells Reason. “Very little that HHS does…is morally defensible, constitutional, and net beneficial to society.”
Indeed, federally funded research is a relatively recent phenomenon. Before World War II, the federal government only financed about one-fifth of the nation’s research and development. The private sector led several successful research projects, including the discovery of a yellow fever vaccine. Today, the private sector still plays a leading role in financing the nation’s R&D, which has led to groundbreaking results in stem cell research and treatments for pancreatic cancer.
But over time, HHS has significantly expanded its size and involvement in people’s everyday lives. As HHS has grown, so too has the national debt, which is one reason why Kennedy is proposing these cuts. As he explained last week: “Nobody wants to cut NIH funding. I don’t want to cut it….But somehow, we’ve got to tighten our belt in order to save our kids” from the impending cost of the national debt, which stands at $31 trillion held by the public.
Unfortunately, Kennedy’s proposed budget cuts barely make a dent; as spending would go down in certain areas, other programs would see their line items increase. This includes spending on nutrition services (which would go up by $19 million), food safety and chemical regulation ($57 million), and infection prevention and food safety programs ($55 million).
As Cannon points out, Kennedy’s penchant for less government intrusion and “Don’t tread on me” freedom, which was on display last week during a heated exchange about raw milk contaminants, is often applied sporadically, rather than universally. “His priorities do not seem to be reducing the size of government.”
Ultimately, it will be up to Congress to enact any of these proposed cuts. This seems unlikely, given the hostility of these hearings, which have shown just how difficult it is to reduce the size of the state. For now, even modest cuts in spending are proving too much for Congress to handle.
The post Lawmakers Seem Unlikely To Back RFK's $16 Billion Cuts to HHS appeared first on Reason.com.
]]>
Under a draft Crown Prosecution Service document in England and Wales, male circumcision could be treated as a possible form of child abuse, placing it in the same category as other “harmful practices” including exorcisms. The proposal has alarmed Jewish and Muslim leaders who say circumcision is an important and generally safe religious tradition.
The post Brickbat: Won't Make the Cut appeared first on Reason.com.
]]>
Under new Food and Drug Administration (FDA) guidance on “low risk” wearable technology and software, AI-powered health tools are rapidly expanding, leading to major implications for cost, access, and consumer autonomy in health care.
One of the clearest examples is Doctronic, an AI-powered platform for prescription refills that rolled out in Utah this month. The FDA has not moved to regulate or stop Doctronic from operating, largely because the FDA does not regulate the actual practice of medicine. That leaves Doctronic free to innovate to patients’ benefit—prescription refills with Doctronic are currently $4 and could fall as the company grows.
Within days of the new FDA guidance, a cascade of other innovations was announced. OpenAI unveiled a waitlist for ChatGPT Health, which offers a platform for users to connect their health data and receive insights. Anthropic, which developed the AI assistant Claude, followed with plans to improve the electronic health records ecosystem with a new product designed to meet federal patient-privacy requirements. “When connected, Claude can summarize users’ medical history, explain test results in plain language, detect patterns across fitness and health metrics, and prepare questions for appointments,” Anthropic announced.
Then, on January 12, OpenAI also announced its purchase of a health tech startup called Torch, which aims to address the continuity problems surrounding “fragmented” patient data. The company is developing a complement to medical record systems by unifying “lab results, medications, and visit recordings,” storing patient records, and centralizing coordination.
Doctronic also announced this week that it’s working on “Checkup by Doctronic,” an AI-powered annual physical that includes bloodwork in addition to Doctronic’s AI prescription refills. That product may be ready as soon as February 1.
These developments are possible because health wearables and software are classified by the FDA based on perceived risk and the nature of their medical claims. Tools such as Doctronic, Viome, Oura Ring, January AI, WHOOP, and Apple Watch are considered low risk rather than moderate risk because they do not diagnose disease or recommend treatment directly. Similarly, Google’s MedGemma 1.5 for medical imaging for 3D CT and MRI analysis is exempt from FDA scrutiny because of its informal designation as a research and development product rather than a clinical tool.
In contrast, non-low risk software such as Natural Cycles, a software application for contraception (the first FDA-approved digital birth control) and Stelo by Dexcom, a glucose tracking monitor, are still regulated by the FDA’s De Novo process for novel moderate-risk devices. Hospital-grade technologies, such as the recently announced Biotics AI fetal ultrasound, are regulated through the 510(k) process, which requires proof of equivalence to an existing device or “predicate.”
The FDA’s deregulatory shift is already producing benefits for innovators and consumers. WHOOP recently announced a partnership with Ferrari as its official digital health wearable. (Just six months ago, WHOOP received a warning letter from the FDA for selling an “unauthorized medical device.”) But now, under the new framework, as long as a device does not claim to be “medical grade,” does not diagnose disease, and remains classified as low risk, it is effectively fair game for market entry.
The FDA’s move might be bigger than getting pills prescribed by an AI doctor: It could help rein in health care spending. “Medical science experts have estimated that ‘widespread AI adoption within the next five years using the technology available today could result in savings of 5% to 10% of healthcare spending, or $200 to $360 billion annually'” according to Adam Thierer of the R Street Institute.
Consumers are demanding access to diagnostics without the politicization of the health environment. Users can already upload their labs to ChatGPT, for example, for analysis and second opinions. Anthropic’s new tool may also be able to draft clinical trial protocols, and Oura Ring is already making clinical trials more accessible to consumers without relying on a clunky and impersonal health care system. In Utah, AI-based prescription refills are already lowering costs and returning autonomy to the health consumer.
If AI-based health software is allowed to flourish, health care costs could plummet, hospital readmission rates might drop meaningfully, and disease could be detected earlier. “Missed prevention is costly for all parties involved, including employers who insure their workforce,” Rachel Curry wrote for CNBC in 2023. “The [Centers for Disease Control and Prevention] says that 90% of the $4.1 trillion in annual health care expenditures are for people with chronic and mental health conditions, and preventative care is considered the key interceptor for chronic conditions.”
By stepping back from strict oversight, the FDA is also saving emerging health tech companies huge amounts in layered costs. As long as AI tools don’t “diagnose disease” and are simply “providing information,” companies have leeway to innovate in the market without prior approval. “We don’t want people changing their medicines based on a screening tool or an estimate of a physiologic parameter,” FDA Commissioner Marty Makary told Fox Business.
Markets and investors want predictability, which is cited by Makary as a reason for the new FDA guidance. Rather than preemptively block innovation, the FDA is allowing competition to determine which tools succeed: “Let’s let doctors choose from a competitive marketplace which ones they recommend for their patients,” Makary said.
The post The FDA's Hands-Off Approach to Medical AI Is a Win for Health-Conscious Consumers appeared first on Reason.com.
]]>
Essilor’s new Stellest lenses—approved by the Food and Drug Administration (FDA) in September 2025—promise to slow nearsightedness in children. They use concentric lenslets to redirect light and reduce myopia progression by up to 70 percent over two years, according to company data.
The lenses are already used across Europe and Asia. The FDA threshold for “reasonable assurance of safety and effectiveness” tends to be especially high, which likely prolonged the review.
The post Photo: These Lenses Can Slow the Progression of Nearsightedness appeared first on Reason.com.
]]>
Defending COVID-19 policies against legal challenges, government officials relied heavily on Jacobson v. Massachusetts, a 1905 case in which the U.S. Supreme Court upheld a smallpox vaccine mandate imposed by the Cambridge Board of Health. But the breadth of the license granted by that decision is a matter of dispute, even as applied to superficially similar COVID-19 vaccination requirements.
Critics of those mandates argued that COVID-19 shots, unlike smallpox vaccination, do not prevent disease transmission, so requiring them amounts to paternalistic intervention rather than protection of the general public. Last summer in Health Freedom Fund v. Carvalho, the U.S. Court of Appeals for the 9th Circuit dismissed that distinction as constitutionally irrelevant.
Rejecting a challenge to a 2021 COVID-19 vaccine mandate that the Los Angeles Unified School District (LAUSD) imposed on its employees, the majority held that the district “could have reasonably concluded that COVID-19 vaccines would protect the health and safety of its employees and students.” The implications of the 9th Circuit’s decision for the right to bodily integrity are alarmingly broad, since the court’s logic would seem to bless all manner of medical mandates that the government views as beneficial to the patient, even if they have no effect on other people.
The plaintiffs in the 9th Circuit case, including LAUSD employees who were fired because they refused to comply with the vaccine requirement, argued that Jacobson did not authorize that policy. Their case featured dueling interpretations of Jacobson that reflected different understandings of “public health.”
Is that rationale for government action limited to external threats such as disease carriers and air pollution, where someone’s actions risk harming others, or does it extend to self-regarding decisions that do not impinge on other people’s rights, such as lifestyle choices and consent to medical treatment? The 9th Circuit’s ruling implicitly embraces the latter view, which invites far-ranging, open-ended interference with individual freedom.
In Jacobson, the Supreme Court weighed “the inherent right of every freeman to care for his own body and health in such way as to him seems best” against the government’s interest in “preventing the spread of smallpox.” The majority repeatedly referred to that danger and noted “the common belief,” supported by “high medical authority,” that vaccination was effective at addressing it. The Court rejected the premise that people may do as they like “regardless of the injury that may be done to others.”
That concern about injury to others, the plaintiffs in the 9th Circuit case argued, did not apply in the context of COVID-19 vaccine mandates. While smallpox vaccination effectively curtailed the spread of disease, they said, COVID-19 vaccines do not prevent infection or transmission, although they may reduce symptom severity in people who receive them.
The LAUSD argued that COVID-19 vaccination does make transmission less likely, or at least that it was reasonable to think so when the mandate was adopted. But initial expectations, based on clinical trials, that the vaccines would effectively retard the spread of COVID-19 were contradicted by real-world experience, especially with emerging variants of the virus.
In 2024, a three-judge 9th Circuit panel deemed that point relevant. The majority noted that Jacobson “did not involve a claim in which the compelled vaccine was ‘designed to reduce symptoms in the infected vaccine recipient rather than to prevent transmission and infection.'”
When an 11-judge panel reheard the case, however, the majority concluded that the LAUSD mandate’s constitutionality depended on “what reasonable legislative and executive decisionmakers could have rationally concluded about whether a vaccine protects the public’s health and safety, not whether a vaccine actually provides immunity to or prevents transmission of a disease.” Since the plaintiffs conceded that COVID-19 vaccines “lessen the severity of symptoms for individuals who receive them,” the court said, the policy easily passed muster.
The majority “suggests that Jacobson‘s reference to ‘public health and public safety’ is so capacious that merely ‘lessen[ing] the severity of symptoms’ is enough to justify a vaccine mandate,” two dissenting judges complained. That logic, they warned, “comes perilously close to giving the government carte blanche to require a vaccine or even medical treatment against people’s will so long as it asserts—even if incorrectly—that it would promote ‘public health and safety.'”
The implications of the 9th Circuit’s decision extend beyond coercive medical treatment. The court’s expansive understanding of “public health and safety” obliterates the distinction between public and private, justifying forcible intervention whenever the government thinks it will protect recalcitrant individuals from disease or injury.
The post Can the Government Mandate a Vaccine for Your Own Good? This Federal Court Says Yes. appeared first on Reason.com.
]]>
Before voting to confirm Robert F. Kennedy Jr. as the secretary of Health and Human Services (HHS), Sen. Bill Cassidy (R–La.) stated on the floor of the Senate that RFK Jr. had promised him that “he would work within the current vaccine approval and safety monitoring systems, and not establish parallel systems. If confirmed, he will maintain the Centers for Disease Control [CDC] and Prevention’s Advisory Committee on Immunization Practices without changes. CDC will not remove statements on their website pointing out that vaccines do not cause autism.”
Every one of the main promises made to Cassidy has been broken. Eschewing the usual system of consultations with outside independent vaccine experts, RFK Jr. announced on X in May that “as of today the COVID vaccine for healthy children and healthy pregnant women has been removed from the CDC recommended immunization schedule.” This announcement makes it harder for expectant mothers to access the vaccines because some insurance companies are less likely to pay for them.
In their lawsuit in response to RFK Jr.’s announcement, the American Academy of Pediatrics, the American College of Physicians, and the American Public Health Association argued that the secretary’s goal is “to undermine trust in vaccines and reduce the rate of vaccinations in this country.”
What about his promise to maintain the CDC’s Advisory Committee on Immunization Practices without changes? Nope. RFK Jr. fired all of the vaccine experts and loaded up the committee with anti-vaccination appointees.
Finally, there is RFK Jr.’s promise that the CDC will not remove statements on its website pointing out that vaccines do not cause autism. As of Wednesday, the CDC website states:
- The claim “vaccines do not cause autism” is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.
- Studies supporting a link have been ignored by health authorities.
- HHS has launched a comprehensive assessment of the causes of autism, including investigations on plausible biologic mechanisms and potential causal links.
After making these statements at the top of the webpage, the CDC website maintains a headline with an asterisk.
Why the asterisk? A note at the bottom of the page explains:
The header “Vaccines do not cause autism” has not been removed due to an agreement with the chair of the U.S. Senate Health, Education, Labor, and Pensions Committee that it would remain on the CDC website.
These changes are not merely dishonest; they are dangerous. All three of the new claims at the top of the CDC website are specious.
First, evidence accumulated over numerous studies, including studies with millions of children, has found no link between vaccinations and autism.
Second, in support of this claim that studies suggesting a link are ignored, the CDC gestures at reviews by the HHS’s own Agency for Healthcare Research and Quality (AHRQ). Scrounging through them for something that might suggest harm, RFK Jr.’s team found a minor note in a 2021 AHRQ report that observed the current evidence for childhood Tdap (Tetanus, diphtheria, pertussis) vaccination is “insufficient to support or reject a causal relationship between those vaccines and autism.”
The report found that with respect to vaccines recommended for children and adolescents, “we found either no new evidence of increased risk for key adverse events with varied [strength of evidence] or insufficient evidence.” The critical question is: “insufficient evidence” for what? The report explains: “There remains insufficient evidence to draw conclusions about some rare potential adverse events [emphasis added].” Certainly, RFK Jr.’s alleged “autism epidemic” caused by vaccines would not count among “rare potential adverse events.”
It is worth noting that the cited 2021 AHRQ report is peppered throughout with findings that vaccines do not cause autism. The new CDC site also fails to mention that the report observed that prenatal Tdap vaccination is not associated with a higher risk of autism in children.
Meanwhile, as a result of falling Tdap vaccination rates, the number of American children infected with whooping cough (pertussis) is surging.
What about the third claim that HHS has launched a “comprehensive assessment of the causes of autism”? In April, RFK Jr. appointed anti-vaccination stalwart David Geier to head up that assessment. As I noted at the time, “Geier will doubtlessly and transparently get the answers that our new secretary of Health and Human Services thinks he already knows.” In September, RFK Jr. announced the dubious finding that taking the painkiller Tylenol during pregnancy was associated with a higher risk of autism in children.
“We are appalled to find that the content on the CDC webpage ‘Autism and Vaccines’ has been changed and distorted,” declares the Autism Science Foundation in a statement, “and is now filled with anti-vaccine rhetoric and outright lies about vaccines and autism.”
That’s correct. This isn’t what the Senate—or the American people—were promised.
The post RFK Jr. Breaks His Promises About the CDC on Vaccines and Autism appeared first on Reason.com.
]]>But numerous studies going back to the year 2000 all indicate there is no particular reason to fear cell phones as a cause of cancer, and a new paper by Li Zhang and Joshua Muscat of the Department of Public Health Sciences at Pennsylvania State University examines the most up-to-date data from the United States to examine this question as if for the first time.
Most studies on this question so far have been case-control studies. This type of study is subject to biases (information bias and selection bias) because it selects subjects who already have the disease of interest (in this case, brain cancer). Although prospective studies avoid the biases inherent in case-control studies, they are expensive and difficult to carry out, especially for rare diseases such as brain cancer.
But now researchers can take advantage of the exponential increase in exposure to cell phones since their introduction in the mid-1980s. In the space of several decades, humans have gone from having no exposure—zero percent of the population exposed—to nearly universal exposure. This means that we can take advantage of what is referred to as a “natural experiment,” the approach that Li and Muscat take in their illuminating new study.
An earlier analysis of this type was carried out by the National Cancer Institute. That study showed no evidence of an association between cell phone use and cancer, but the data only went up to 2012. Possibly cell phones had not been in use long enough for an effect to show up. Li and Muscat extend the period of observation by nine years.
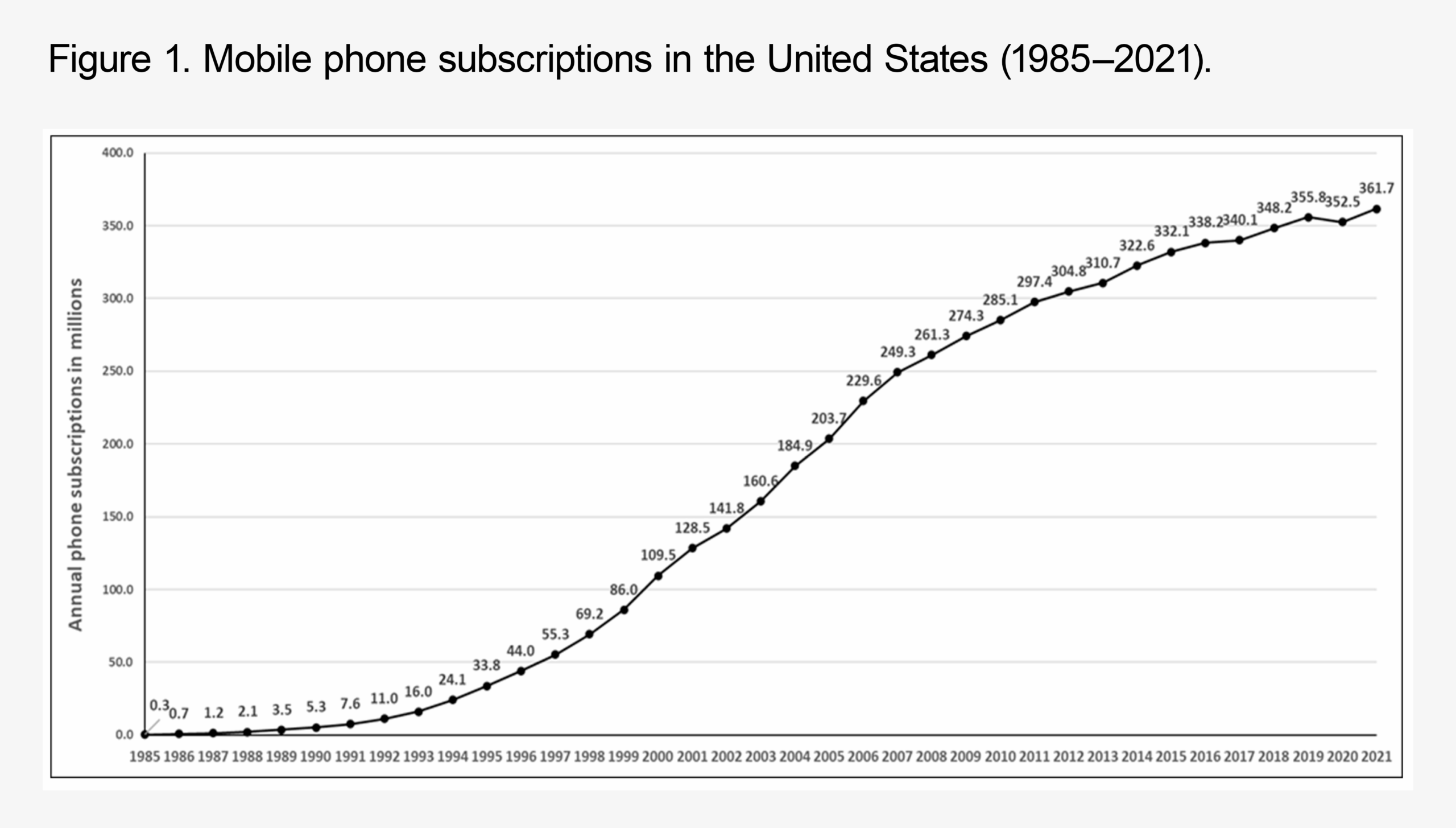
The authors plotted the total number of cell phone subscriptions in the U.S. for the period 1985-2024 and used data on brain cancer and brain tumor incidence from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program for the years 2000 to 2021 to calculate the annual percentage change (APC) in the incidence of brain cancer and non-malignant tumors of the brain. The SEER database for this period covers 47.9 percent of the U.S. population.
From 1985 to 2021, there was a 1,200-fold increase in the number of cell phone subscriptions in the United States (Figure 1).
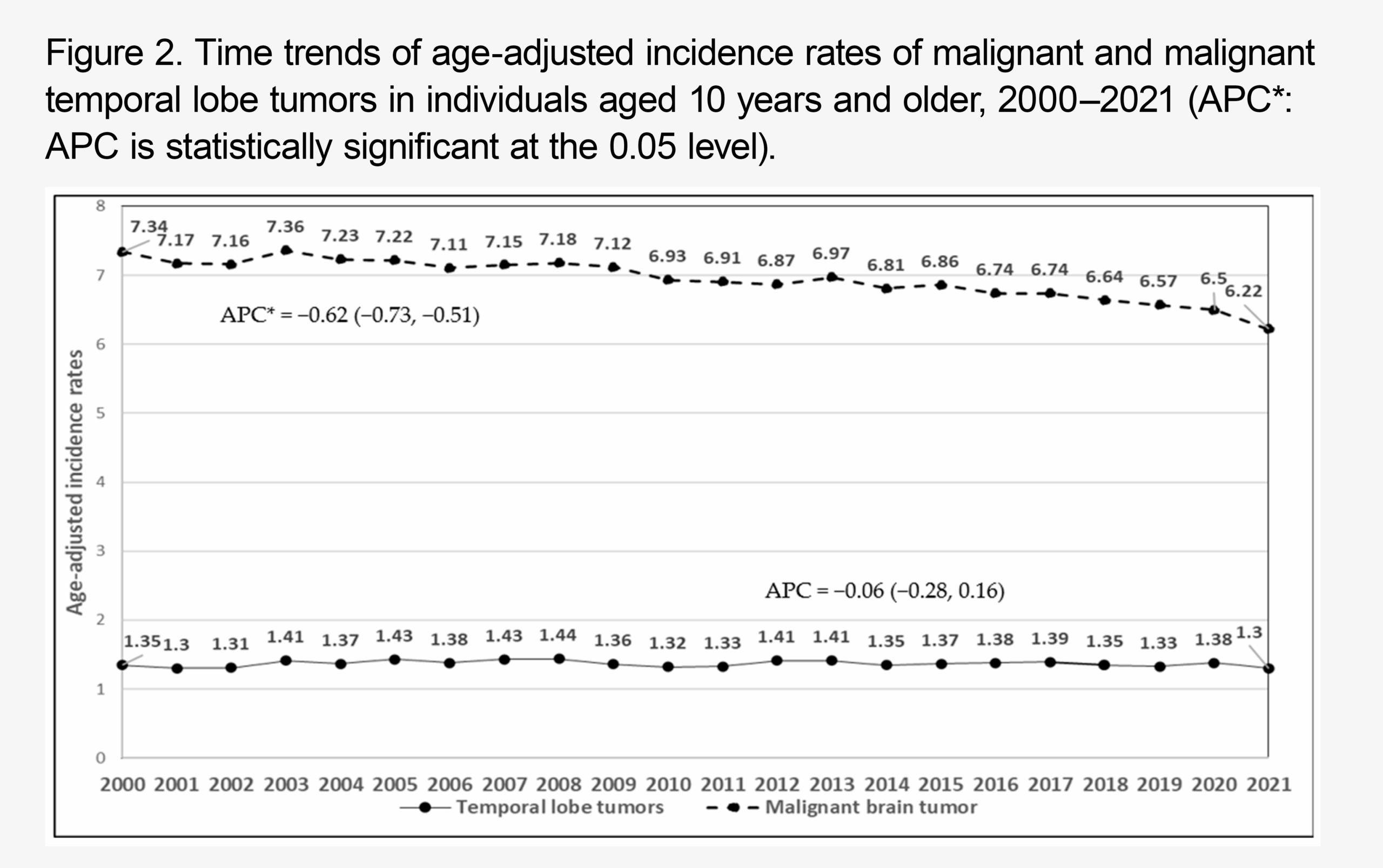
Along with this dramatic increase in cell phone use, a slight decline in annual percent change for malignant brain tumors occurred, and no change in temporal lobe tumors appeared from 2000 to 2021 (Figure 2).
There was a slight increase in benign tumors (mainly meningiomas), but this is likely to be due to an increased use of medical imaging during this period discovering tumors that earlier would have gone undetected.
For acoustic neuromas (vestibular schwannomas), malignant pediatric brain tumors, and pediatric temporal lobe tumors, there was no evidence of an increase over the 21-year period.
The authors conclude that “these findings suggest that mobile phone use does not appear to be associated with an increased risk of brain cancer, either malignant or benign.”
Notice how restrained their language is. As the authors point out, their results are in agreement with those from previous studies using different methodologies and carried out in different countries, including the United Kingdom, Scandinavia, New Zealand, Europe, and the United States. These studies have generally found no evidence of an association between cell phone use and cancers.
The extensive null evidence from epidemiologic studies needs to be seen in conjunction with what is known from biophysics about the effects of exposure to radiofrequency energy emitted by cell phones. Unlike ionizing radiation, such as X-rays, radiofrequency energy has much longer wavelengths and much lower frequencies that are too weak to break chemical bonds or damage DNA. There is no evidence that these waves can initiate cancer.
Thus, different types of evidence all converge to indicate that cell phone emissions are unlikely to cause cancer.
I have summarized these findings—from the most recent study and from studies going back 25 years—to show how, as more studies are done and attempts are made to improve the quality of the data, we can be more and more certain that these studies are sound and that we are not missing something.
I have gone on at length about cell phones in order to contrast the slow, steady, and disciplined conduct of science with the corrosive disinformation that is being put out on a daily basis by RFK Jr., who leads the largest biomedical agency in the United States and in the world.
As is the case with cell phones, the available scientific evidence indicates that there is no association between vaccines, and specifically the MMR vaccine, and autism. In fact, the evidence for vaccines not causing autism is even stronger than the evidence for cell phones not causing brain cancer. This is because, for vaccines, we have very high-quality data on the exposure of individuals (the type of vaccine, the dose, the date of vaccination). And we have this information on millions of children. This means that we can have very strong confidence that vaccines do not cause autism.
And yet, in the face of this evidence, RFK Jr. insists on propagating this debunked claim, and he is sponsoring a study by a discredited researcher that he hopes will provide the answer he favors. This is an unforgivable waste of money that could be spent on addressing an important health issue. But it is also more than that.
From observing RFK Jr., and those he appeals to, we see that the belief in different bogus claims tends to be correlated. A belief that cell phones are causing cancer or that vaccines cause autism can serve as a sentinel indicator of the susceptibility to other false beliefs, such as those targeting pesticides and genetically engineered crops. It’s noteworthy that the prominent anti-biotech advocacy organization U.S. Right-to-Know is anti-vaccine in addition to being fiercely against glyphosate and other pesticides and genetically modified crops.
These, and many others, are zombie risks that never die. It doesn’t matter what the specific risk is. The credulity, the failure to take any commonsense evidence or distillations of the scientific evidence into account, the refusal to value the judgment of experts who have spent untold hours examining the issue, or the conclusions reached by institutions such as the National Institutes of Health, the Institute of Medicine, or the American Cancer Society, into account are the same.
RFK Jr. appears to have an implacable drive to do away with vaccines by undermining public confidence, disrupting insurance coverage, and making it too costly for pharmaceutical companies to produce them, as happened in the 1980s. Exposing his lies is literally a matter of protecting the lives of children and adults from the all-too-real infectious diseases that RFK Jr. doesn’t believe in.
Editor’s note: RFK’s various quirks and mistakes are analyzed at length in Reason‘s July cover story by Elizabeth Nolan Brown on his Make America Healthy Again movement, and will be discussed tonight, Wednesday, June 25, in a Reason Speakeasy event featuring Brown and hosted by Nick Gillespie at the Blue Building, located at 222 East 46th Street in Midtown Manhattan. Doors open at 7 p.m., and Nick’s conversation with Brown will begin at 7:30 p.m., followed by audience Q&A and a reception. Tickets include beer, wine, soft drinks, and a selection of healthy and unhealthy appetizers.
The post Despite What Robert F. Kennedy Wants You To Think, Cell Phones Do Not Cause Brain Cancer appeared first on Reason.com.
]]>Sen. Josh Hawley (R–Mo.) seems to agree. The day the Ethics & Public Policy Center (EPPC) released its new mifepristone study, Hawley wrote to Food and Drug Administration (FDA) chief Marty Makary, urging the commissioner to “follow this new data and take all appropriate action to restore critical safeguards on the use of mifepristone.”
Makary said in late April that he has “no plans” to restrict access to abortion pills. But he added that “there is an ongoing set of data that is coming into FDA on mifepristone. So if the data suggests something, or tells us that there’s a real signal, we can’t promise we’re not going to act on that data that we have not yet seen.”
Taken at face value, that’s simply a reasonable statement of scientific uncertainty. But it seems a little odd considering we have decades of data on mifepristone already—this isn’t some new or relatively unstudied drug. And things get even dicier when we consider that, a few days after Markary’s April 24 comments at the Semafor World Economy Summit, a conservative group released new data that are being used by conservative politicians to suggest it is time for the FDA to act.
The Study
Hall and Anderson base their arguments on their claim that “serious adverse events” are very common with mifepristone—occurring, they say, in slightly more than a tenth of patients.
They based this conclusion on information gleaned from an insurance claim database. It contained “de-identified data for all U.S. patients during the years 2017 to 2023,” and they identified 865,727 likely mifepristone-enabled abortions in this database. Of these cases, 10.93 percent ended in a “serious adverse event,” they say.
Clinical trial reports of a “less than 0.5 percent” adverse event rate are way off, they conclude—and therefore, they argue, mifepristone is neither safe nor effective.
But the methods they used to reach these conclusions are highly questionable.
First, they identified “mifepristone abortions” by flagging insurance codes indicating the prescription of mifepristone with or without misoprostol, a “medically induced abortion by oral ingestion of medication,” or the “elective termination of pregnancy” in conjunction with billing codes that suggest mifepristone was given.
Already there are problems. This study is supposed to concern the safety of people undergoing a drug-induced abortion, right? But people who have miscarried naturally are also prescribed mifepristone, and they seem to be lumped in here, despite the fact that they have different circumstances that could wind up producing more, fewer, or different sorts of adverse events than seen in patients prescribed the drug for elective abortion in the first 10 weeks. Furthermore, the authors do not seem to take into account whether patients followed up the mifepristone with misoprostol, as is the FDA’s recommended practice. Taking mifepristone alone might lead to different outcomes than seen with the two-pill protocol.
And then there’s a much bigger issue—what the study considers a “serious adverse event.”
There’s a clear pattern in the study, in which the very specific or clearly dire categories of adverse events occurred in a relatively small number of patients, while the categories that make up the bulk of adverse events flagged are vaguely defined and may represent minor or even benign situations.
Just 0.10 percent of cases resulted in patients getting sepsis, 0.15 percent ended in patients needing blood transfusions, and 0.22 percent in what the study authors define as other life-threatening events.
The rates of serious and well-defined complications here are all low and well within the parameters advertised by abortion pill manufacturers. The reason this study finds so much higher prevalence of adverse events comes down to the event categories they won’t tell us much about.
Emergency Room Visits and ‘Other’ Complications
Of the 865,727 cases analyzed (some of which involved repeat patients), 94,605 were determined by the authors to have ended in serious adverse events, which they defined as any one of a broad range of outcomes happening within 45 days of taking the pill.
Patients could be coded into multiple categories, so someone admitted to the hospital for an infection might be listed in both the infection and hospitalization categories.
The largest category of adverse events is “other abortion-specific complications,” reportedly experienced in 49,169 cases. But the authors give us little idea about what these “other” complications might be. By definition, they do not include sepsis, infection, transfusion, hemorrhage, an ectopic pregnancy, a need for a surgical abortion, or “other life-threatening events.” The only explanation the authors give is that “other abortion complications include codes specifically related to an abortion or miscarriage, as well as life-threatening mental health diagnoses, etc.”
And this seems all the more questionable when they allude to an undefined category of “mental health” issues that occur within a month and a half after taking the pill.
“Let’s say you go see your doctor for anxiety or insomnia a month after having an abortion,” writes Jessica Valenti in the Abortion, Every Day newsletter. “Because EPPC is counting any event that happens within 45 days of taking mifepristone—and they’re not defining ‘life-threatening’—your sleep problem or anxiety could be counted as a ‘serious adverse event’ of abortion pills.”
It also seems possible that some situations—sexual assault, relationship troubles, a wanted pregnancy with fetal anomalies, health problems, money problems—could trigger both a desire for an abortion and some mental health problems. In those cases, it would hardly be the pill itself that is to blame. And even if the mental health issues flagged were directly related to feelings about the abortion, it still hardly seems fair to describe them as serious complications stemming from the pill itself.
The study’s second biggest category of adverse events is listed as emergency room visits, experienced in 40,960 cases. This category also suffers from some lack of information, as an emergency room visit alone does not actually tell us whether a serious complication took place.
Women who take mifepristone often start experiencing the pill’s effects outside of the normal business hours of an doctor’s office or health clinic. Some might go to the emergency room to check on levels of pain or bleeding that turn out to be normal.
Without actually knowing the nature and outcome of the emergency room visits in this study, we can’t conclude much of anything. The fact that there were more than 40,000 trips to the emergency room but far fewer hospitalizations—5,699—suggests that many of these visits did not result in serious risks or harms.
For what it’s worth, the FDA has said that emergency room visits in themselves are not enough to count as serious adverse events. The agency defines serious adverse event as death, hospitalization, anything life-threatening, anything resulting in disability or permanent damage, anything requiring medical or surgical “intervention to prevent permanent impairment or damage,” and anything that “may require medical or surgical intervention…to prevent one of the other outcomes.”
Drilling Down Further
The third largest category of adverse events in the EPPC study is “hemorrhage,” which occurred in 28,658 cases. Hemorrhages can be quite serious, of course. But “even that [hemorrhage] data is suspect because the EPPC doesn’t define what it means!” writes Valenti. “Doctors I spoke with say bleeding is expected during medication abortion, and it’s only considered a serious complication if a blood transfusion is needed.”
Transfusions were needed in far fewer cases (1,257) than there were cases of hemorrhage. The discrepancy in numbers here draws into question whether all of the events counted in the hemorrhages category should really be deemed serious adverse events. (Again, we could be looking at women who sought medical attention for what turned out to be normal amounts of bleeding.)
The fourth largest category of adverse events was needing a surgical abortion after taking the pill, happening in 24,593 of the cases. But it’s a well-advertised fact that the two-pill regimen is successful in only about 87 to 98 percent of cases, depending on when in pregnancy the mifepristone and misoprostol are taken.
If fewer than three percent of people in the study needed surgical abortions after taking mifepristone, that is well within the expected range and not necessarily a sign of anything unusual. It simply means these drugs, like many drugs, are not 100 perfect effective.
The smallest category of adverse events in the EPPC analysis was sepsis, a life-threatening infection that occurred in 824 cases.
Far more people suffered from some sort of infection—11,707 cases, or 1.34 percent.
Again, with infections, we have a category where it’s hard to know what exactly is meant. Infections here may include yeast infections, urinary tract infections, or minor vaginal bacterial infections—things that may be unpleasant but aren’t generally serious unless left untreated and aren’t necessarily the fault of taking the pill per se. Having sex, using tampons, or engaging in other not-recommended behaviors too soon after an abortion or miscarriage can result in infections.
The remaining categories were ectopic pregnancy (something not caused by abortion pills but a situation in which abortion pills will not work and would not be recommended), in 3,062 cases; and “other life-threatening adverse events,” in 1,956 cases.
Bad Data Makes Bad Policy
Perhaps aware that total revocation of FDA approval isn’t in the cards (yet), Hawley told Makary it “is time to revisit and restore the FDA’s longstanding safety measures governing mifepristone.”
Over the past decade, the FDA has relaxed its rules around mifepristone prescribing, now allowing it to be prescribed up to 10 weeks into a pregnancy (instead of the former seven weeks), to be prescribed remotely, and to be shipped by mail. Those last two changes seem especially to anger anti-abortion advocates, since they help women in states where abortion pills are illegal in obtain them from doctors and pharmacies in states where they are not.
Advocates previously tried to get the courts to change those requirements. The matter went all the way to the U.S. Supreme Court, but it rejected the challenge, holding that those who brought the case didn’t have standing to do so. And while the same issues could be raised by a different group of plaintiffs, the standing problem could prove difficult to overcome.
That means that changing the national rules regarding the prescription of mifepristone and misoprostol may have to rely on persuading the FDA to change its policy. So that’s what the EPPC is trying to do.
“The FDA should reinstate the original patient safety protocols that were required when mifepristone was first approved,” write the study’s authors, Jamie Bryan Hall and Ryan T. Anderson. “Doing so will likely reduce the harms to women and permit better monitoring to determine whether this drug should remain on the market.”
They argue that getting mifepristone “should require at least three in-person office visits by the patient,” that it should be prescribed only by physicians (some states allow prescription by nurse practitioners, physician’s assistants, or certified midwives), that it should have to be taken in a medical facility, that it should be allowed only through the first seven weeks of pregnancy, and that prescribing physicians “must be able to provide surgical intervention in cases of incomplete abortion or severe bleeding, or have made plans to provide such care through others, and be able to assure patient access to medical facilities equipped to provide blood transfusions and resuscitation, if necessary.” Rule changes such as these would make it highly difficult for women in states where abortion is illegal to access abortion-inducing drugs outside of the black market.
The fact that so much of this study was worded so vaguely should give everyone pause. If all of the serious adverse events cited here were undeniably serious, the researchers should have no problem defining them concretely or making their datasets public. That’s the only way to reassure readers that they aren’t inflating their count with less serious health problems.
It would be silly to argue that medication abortion is 100 percent safe. But to put the serious complications in perspective, we should also look to complication rates in pregnancy and in miscarriages. No matter how a pregnancy ends, a pregnant woman incurs some risk. (For the record, “maternal sepsis occurred in 0.04% of deliveries in the United States,” according to research published in the Journal of the American Medical Association in 2019.)
It’s also silly to contrast mifepristone’s current complication rates with some mythical future in which far fewer of these abortions would take place. The alternative to legal and accessible mifepristone isn’t necessarily “no abortion” and “no complications.” It’s also abortion with black market mifepristone or misoprostol pills, abortion attempts through more dangerous means, and abortions in which women feel afraid to seek care if they experience complications.
More Sex & Tech News
Jury selection starts today in the OneTaste trial. Nicole Daedone, founder of the orgasmic meditation company OneTaste, and Rachel Cherwitz, the company’s former head of sales, are charged with one count of conspiracy to commit forced labor and no underlying forced labor charge. Read more about the weak, weird case against them here.
More nuanced findings about teens and tech. Politicians and anti-tech activists like to pretend that research overwhelmingly shows negative findings when it comes to young people and social media. But more and more we’ve been seeing studies that challenge this conventional wisdom, aloing with mixed messages and nuanced feelings from young people themselves.
So it goes in a recent survey from the Pew Research Center. “Our latest survey of U.S. teens ages 13 to 17 and their parents finds that parents are generally more worried than their children about the mental health of teenagers today,” Pew reports.
Moreover, kids are more worried about the way social media might effect other kids’ health than their own—a sign while they might buy into the dire warnings about teens and tech that are all around them, they don’t necessarily find this concern validated by their own experiences:
Roughly half of teens (48%) say these sites have a mostly negative effect on people their age, up from 32% in 2022. But fewer (14%) think they negatively affect them personally.
Meanwhile, 28 percent of the teens surveyed said social media has a mostly positive effect on their own lives, and the majority—58 percent—said it’s neither negative nor positive. And while teens see some ways social media affects them negatively, most notably in terms of sleep and productivity, they also cite it as a source for socialization, creativity, and learning about mental health.
The return of the App Store Accountability Act. This newsletter covered a previous version of this bill last year. Like last year’s iteration, this one would make digital marketplaces, such as Google Play and Apple’s App Store, verify user agers and require parental consent before minors can download apps. Several social media companies, including Meta, Snap, and X, “have endorsed the idea of making app stores a sort of central clearinghouse for age verification,” reports CNN. Apple and Google are opposed.
NetChoice sues over Georgia’s social media age-check mandate. Georgia’s Senate Bill 351 would require social media platforms to “make commercially reasonable efforts to verify the age of account holders,” require parental consent before anyone under age 16 can have an account, and ban targeted advertising to minors. In a new lawsuit, the tech trade group NetChoice argues that the law is unconstitutional. “NetChoice has already permanently blocked similar laws in Arkansas and Ohio because these heavy-handed government mandates violate the First Amendment,” the group explains. “Georgia’s law is no different.”
Today’s Image
The post The Bad Data Backing Josh Hawley's Attack on Abortion Pills appeared first on Reason.com.
]]>